Fixing a failed implant procedure in a single visit
Improper placement of dental implants can severely impact a patient’s health and well being. While there are dentists who can successfully perform placement of dental implants, there are occasions when a dentist should hand off a case to a more experienced implantologist. The following is a review of a failed implant procedure performed by a dentist and how Dr. Mark successfully completed the case.
Dr. Andrei Mark is frequently asked to do second opinions on difficult dental implant cases. Most often this is the case when implants fail or are placed improperly. This was true in the case when a 53-year patient visited Dr. Mark after she had two front teeth extracted (#8 and #9) followed by bone grafting and placement of two implants. She was very unhappy because one implant fell out (#8) and she was very unsure about the remaining implant (#9).
Diagnosing the case
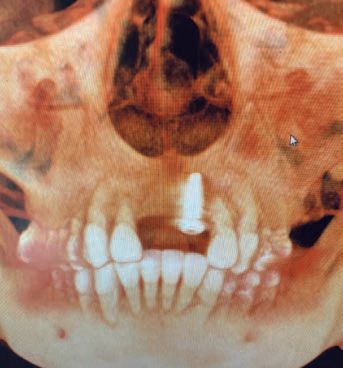
After taking a CAT screen Dr. Mark noticed that #9 was not placed in bone but was free floating in the soft tissue (Figures: A, B) and it too would fail. The patient informed Dr. Mark that she was told that she would need more bone grafting followed by another six months of waiting before new implants could be placed by the original dentist. Commenting on the proposed treatment plan, Dr. Mark said: “Upon examination of the patient and detailed review of the 3D anatomy of the anterior region of the maxilla, I concluded that a ridge splitting technique would be the best option moving forward.” He went on to inform the patient that if the ridge spitting was successful, he would be able to place the implants at the same time. The patient agreed to the procedure and was amazed that the entire process could be completed in one visit.
The procedure
“On the day of the procedure, we anesthetized the patient and opened a large flap in the interior region with horizontal and two vertical releases,” said Dr. Mark. “I located the vertical releases two teeth away from the area where I would operate to allow for a tension-free flap post surgery. The failing implant could be clearly seen touching the surface of the bone (Figure: C) which was then removed without incident.
Detailing the ridge splitting Dr. Mark said: “Using a piezo-electric surgical instrument, a clamshell-type incision was made with two vertical releases near teeth #7 and #10. A horizontal incision was then made through the crestal bone to a depth of about 11 mm creating an oyster-like cavity which can be expanded with dilators, chisels and osteotomies.” (See Figures: D, E, F).
Once the chisels and dilators were used, Dr. Mark now spread the opening to a width of 2 – 3 mm due to the elasticity of the bone. “This allowed plenty of room for placement of two MIS 3.75 x 11.5 mm implants (Figures: G, H) which were completely encased in the new boney architecture,” says Dr. Mark (Figures: I, J). “The incisions made in the bone were covered with platelet-rich fibrin and granular, mineralized cortical bone (Figure: K) to create a scaffold for the development of new anatomy.”
The entire surgical site was then covered with PRF membrane created from the blood spin and the flap was released from tension and sutured tension free. The patient returned a week later for a follow up and was healing nicely (Figure: L). Three months later the patient returned to prepare the implants for the final restoration (Figure: M).
The caution
A growing number of dentists looking to grow their practice are placing dental implants themselves. Without the proper training, experience and diagnostic tools, a dentist may risk harm to his patient and practice with a failed implant procedure. One failed procedure could result in malpractice litigation that could ruin a practice. In a study of 242 dental malpractice cases, 24 were dental implant cases—23 of which were performed by general dentists and the remaining one by a periodontist. Given this fact, it would be the course of wisdom to consult with a more experienced implantologist when encountering a case that resides outside of your comfort zone. ■